
Posterior vitreous detachment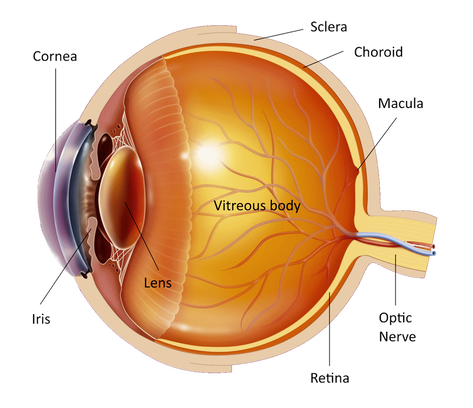
The eye is like a photographic camera. It has the lens and an opening in front that help in the focusing of the objects on the retina. The retina is a thin membrane that is sensitive to the light, as the film in the photographic camera. The macula is found in the center of the retina, where the light focuses. It is responsible for what we see in front of us, for activities such as writing and reading and for the perception of colors. The rest of the retina is responsible for the peripheral vision.
The cavity in front of the retina is full of a transparent jelly like substance that is called vitreous body and takes up about 80% of the volume of the eye. In birth and at young age the vitreous is compact and homogeneous but with aging it starts shrinking and becoming liquid and as a result of this it finally gets detached from the retina. This process is called "posterior vitreous detachment" and normally happens to most people between 40 and 70 years of age. Posterior vitreous detachment may happen earlier to people with myopia or those that have been operated for cataract. As the vitreous detaches from the retina may cause symptoms like floaters. They appear in front of the eye like small dots or curly lines that are moving with the eye. They may give the impression of real flies and are fibrous tissue that is removed from the optic nerve during the posterior vitreous detachment. Flashes are also a common symptom of a posterior vitreous detachment. They are due to traction and stimulation of the retina by the vitreous as it detaches. If during the traction a blood vessel breaks than we can have a vitreous hemorrhage. If the quantity of blood is small it appears suddenly as a rain of small black dots. More blood may reduce the vision considerably. 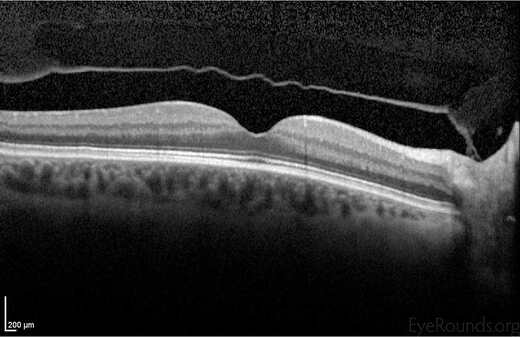
During posterior vitreous detachment a small hole may be formed on the retina to areas of strong vitreoretinal adhesion or to areas where the retina is weak. Then it is likely that fluid vitreous may pass through the hole and under the retina and cause a "retinal detachment". Because posterior vitreous detachment precedes most retinal detachments, it has high importance and must be given considerable attention when it happens.
The recognition of the symptoms of posterior vitreous detachment is the first and most important step towards prevention of retinal detachment. If you have new symptoms (suddenly many floaters, flashes) you will have to be examined by an ophthalmologist as soon as possible. First he will measure your vision in both eyes. Then drops will be put in your eyes to dilate the pupil and examine the retina. You'll have to wait about half an hour for the drops to work. You will have blurred vision for a few hours and you will be sensitive to the light afterwards and therefore you should not drive home after the examination. Then a special contact lens will be put on your cornea to examine the retina and the macula. Your ophthalmologist may also examine you by putting a magnifying lens in front of your eye, wearing a special hat with a light source on his head and pressing your eye with a special instrument. The purpose of these tests is to find all the hole(s) on the retina. Sometimes ultrasound is useful to establish the status of the vitreous and to identify the retinal hole(s). Fortunately, most posterior vitreous detachments do not create retinal holes and only a small portion of retinal holes will eventually lead to retinal detachment. However, if a retinal hole is related to a symptomatic posterior vitreous detachment there is a high likelihood of retinal detachment development and it should be treated. The treatment consists of laser or freezing of the hole under local anesthetic. Sometimes, posterior vitreous detachment, retinal hole and retinal detachment may appear without any previous symptom. And some other times you may have many bothersome symptoms without a retinal hole. Ιf you have any questions about your disease or its treatment do not hesitate to consult you doctor, who will discuss it in details with you. |
The information provided in this web site is not a substitute for professional medical care by a qualified doctor or health care professional. Always check with your doctor if you have concerns about your eye condition or treatment. The authors of this web site are not responsible or liable, directly or indirectly, for any form of damages whatsoever resulting from the information contained in or implied by the information on this site. Information for patients is provided only as a guide.
Copyright Vlassis Grigoropoulos © 2020
Copyright Vlassis Grigoropoulos © 2020






|
Design: Vlassis Grigoropoulos